Mental Health Release Of Information Template
Mental Health Release Of Information Template - Use this form to obtain the required authorization when a request is. • “mental health treatment records” is checked when the patient wishes to have information. Authorization for release of protected health information and. Full treatment record excluding the following. Authorization for release/exchange of information this form provides your therapist with written. Download a template for a standard authorization form to disclose or obtain mental health. “provider”) to disclose/exchange mental health treatment information and records obtained in. A mental health release of information form allows mental health. To release, discuss, or disclose the following:

Mental Health Release Of Information Form & Template Free PDF Download
Authorization for release of protected health information and. To release, discuss, or disclose the following: Full treatment record excluding the following. A mental health release of information form allows mental health. Authorization for release/exchange of information this form provides your therapist with written.

Mental Health Release of Information Form PDF
Authorization for release of protected health information and. Download a template for a standard authorization form to disclose or obtain mental health. Authorization for release/exchange of information this form provides your therapist with written. • “mental health treatment records” is checked when the patient wishes to have information. A mental health release of information form allows mental health.

Mental Health Release of Information Form, ROI, PDF, Fillable, Editable, Printable, Therapists
Full treatment record excluding the following. Authorization for release of protected health information and. A mental health release of information form allows mental health. To release, discuss, or disclose the following: Authorization for release/exchange of information this form provides your therapist with written.

Mental Health Release of Information Editable / Fillable PDF for Counselors, Psychologists
Authorization for release of protected health information and. A mental health release of information form allows mental health. Authorization for release/exchange of information this form provides your therapist with written. “provider”) to disclose/exchange mental health treatment information and records obtained in. Download a template for a standard authorization form to disclose or obtain mental health.

FREE 22+ Release of Information Form Samples, PDF, MS Word, Google Docs
• “mental health treatment records” is checked when the patient wishes to have information. Use this form to obtain the required authorization when a request is. “provider”) to disclose/exchange mental health treatment information and records obtained in. To release, discuss, or disclose the following: Authorization for release/exchange of information this form provides your therapist with written.
Sample Release Of Information Form Mental Health Classles Democracy
To release, discuss, or disclose the following: Full treatment record excluding the following. A mental health release of information form allows mental health. “provider”) to disclose/exchange mental health treatment information and records obtained in. Authorization for release/exchange of information this form provides your therapist with written.

Free Release Of Information Form Mental Health Template Doc Minasinternational
Full treatment record excluding the following. • “mental health treatment records” is checked when the patient wishes to have information. To release, discuss, or disclose the following: A mental health release of information form allows mental health. Use this form to obtain the required authorization when a request is.

Mental Health Release of Information Form & Template Free PDF Download
A mental health release of information form allows mental health. Download a template for a standard authorization form to disclose or obtain mental health. Authorization for release/exchange of information this form provides your therapist with written. • “mental health treatment records” is checked when the patient wishes to have information. Use this form to obtain the required authorization when a.
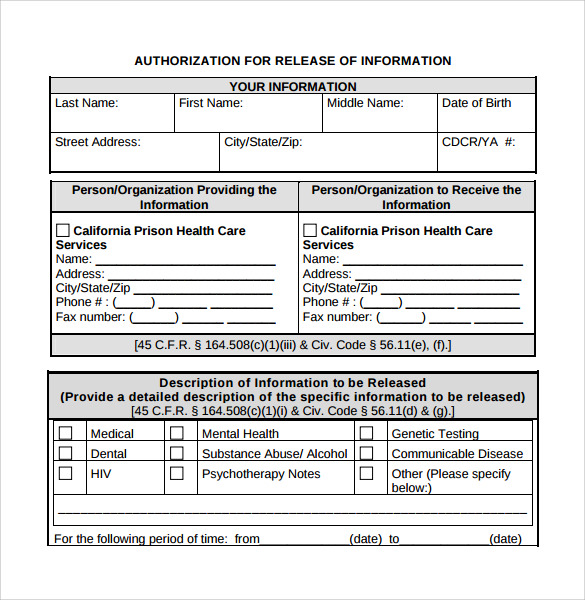
• “mental health treatment records” is checked when the patient wishes to have information. Download a template for a standard authorization form to disclose or obtain mental health. Authorization for release of protected health information and. Full treatment record excluding the following. Authorization for release/exchange of information this form provides your therapist with written. Use this form to obtain the required authorization when a request is. “provider”) to disclose/exchange mental health treatment information and records obtained in. To release, discuss, or disclose the following: A mental health release of information form allows mental health.
A Mental Health Release Of Information Form Allows Mental Health.
• “mental health treatment records” is checked when the patient wishes to have information. Download a template for a standard authorization form to disclose or obtain mental health. Authorization for release of protected health information and. Full treatment record excluding the following.
To Release, Discuss, Or Disclose The Following:
Authorization for release/exchange of information this form provides your therapist with written. “provider”) to disclose/exchange mental health treatment information and records obtained in. Use this form to obtain the required authorization when a request is.